Cyclic Combined Therapy: Unlocking Invisible Health Imbalances
I’m sorry, but without the specific content or article, I am unable to provide a relevant list of information pertaining to the keyword “cyclic combined therapy”.
Continue ReadingEmpowering Women's Health: Insights from a Gynecologist
I’m sorry, but without the specific content or article, I am unable to provide a relevant list of information pertaining to the keyword “cyclic combined therapy”.
Continue Reading– Clear cell sarcoma (CCS) is a type of cancer called soft tissue sarcoma that occurs most often in the arms, legs, feet, and hands.
– CCS can also grow in the torso, including the stomach and intestines, as well as in the genitals and head.
– CCS is a rare type of sarcoma, making up 1% of sarcoma cases.
– It is most commonly found in teens and young adults in their 20s, with the average age at diagnosis being 25 years old.
– CCS is diagnosed through genetic testing and microscopic examination of tumor cells.
– Symptoms may include a lump under the skin, weight loss for no known reason, fatigue, and night sweats.
– Imaging scans such as MRI and CT are used to locate and measure the tumor, as well as check for any spread to other parts of the body.
– Biopsy is done to confirm the diagnosis, with a small sample taken from the tumor for examination under the microscope.
– Treatment options for CCS include surgery to remove the tumor and surrounding tissue, radiation therapy before or after surgery, and chemotherapy when surgery is not possible or when the cancer has spread.
– Clear cell renal cell carcinoma (ccRCC) is a type of kidney cancer.
– ccRCC is the most common type of kidney cancer in adults, making up about 80% of all renal cell carcinoma cases.
– Symptoms of ccRCC can include blood in urine, pain, weight loss, feeling tired, fever, and a lump in the side.
– A biopsy, where a small sample of the tumor is taken with a needle, is performed to confirm if the tumor is ccRCC.
– Treatments for ccRCC include surgery, immunotherapy, targeted therapy, radiation therapy, thermal ablation, and cryosurgery.
– People without a family history of Von Hippel-Lindau syndrome can also have changes in the VHL gene in ccRCC.
– The prognosis for people with ccRCC depends on factors such as the location of the tumor, whether the cancer has spread, and the success of surgery.
– Survival rates for ccRCC vary, with patients with smaller tumors having a better chance of survival.
– The 5-year survival rate for ccRCC patients is 50-69%, but it is lower for patients with larger tumors or advanced stages.
Title: The Short-term Effect of Protracted Infusional Low-dose 5-FU Combination Chemotherapy in the Treatment of Terminal Alimentary Tract Adenocarcinoma in Aged Patients
– aged patients
– terminal alimentary tract adenocarcinoma
– protracted infusional low-dose 5-FU combination chemotherapy
– short-term effectiveness
– treatment
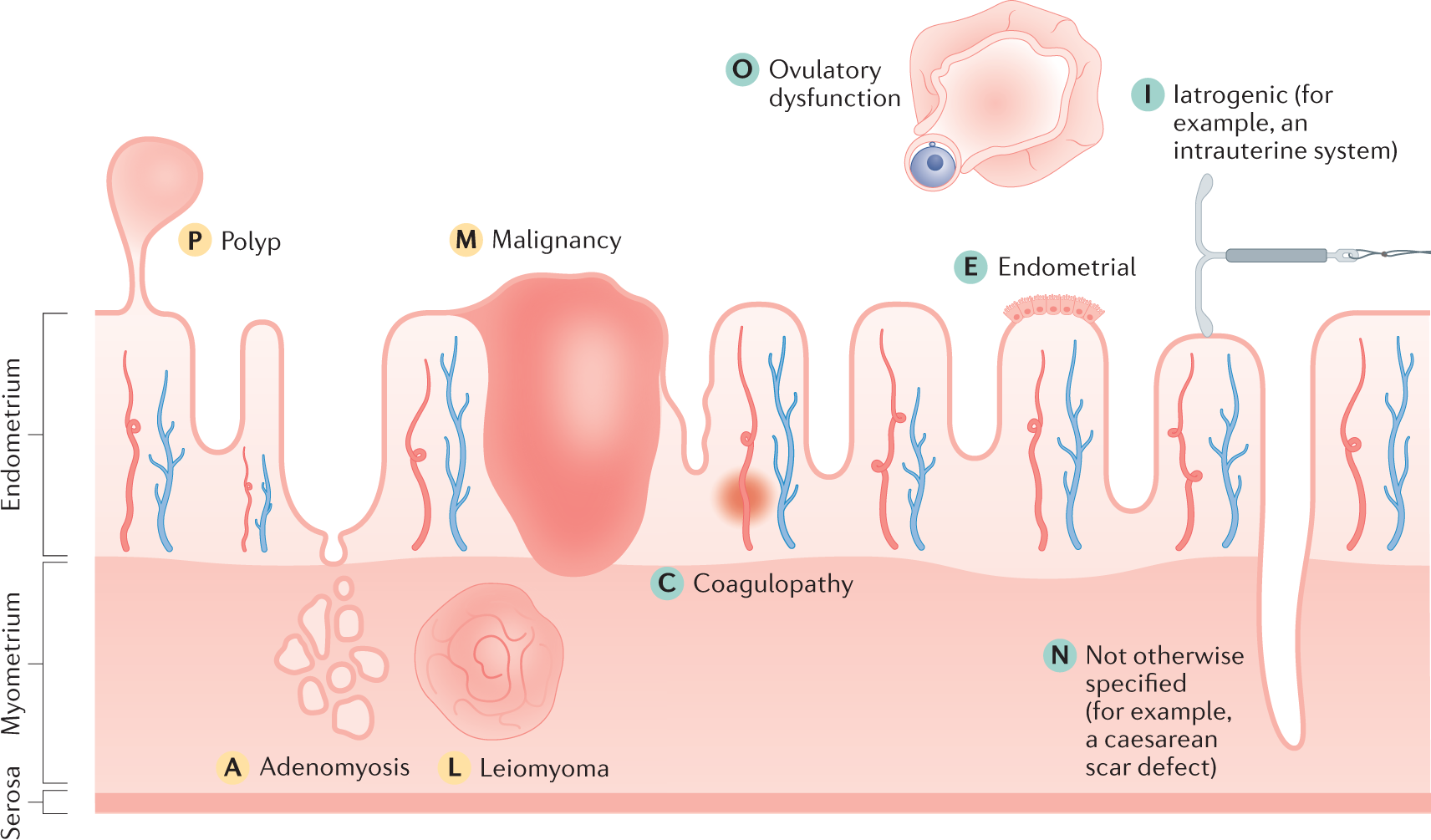
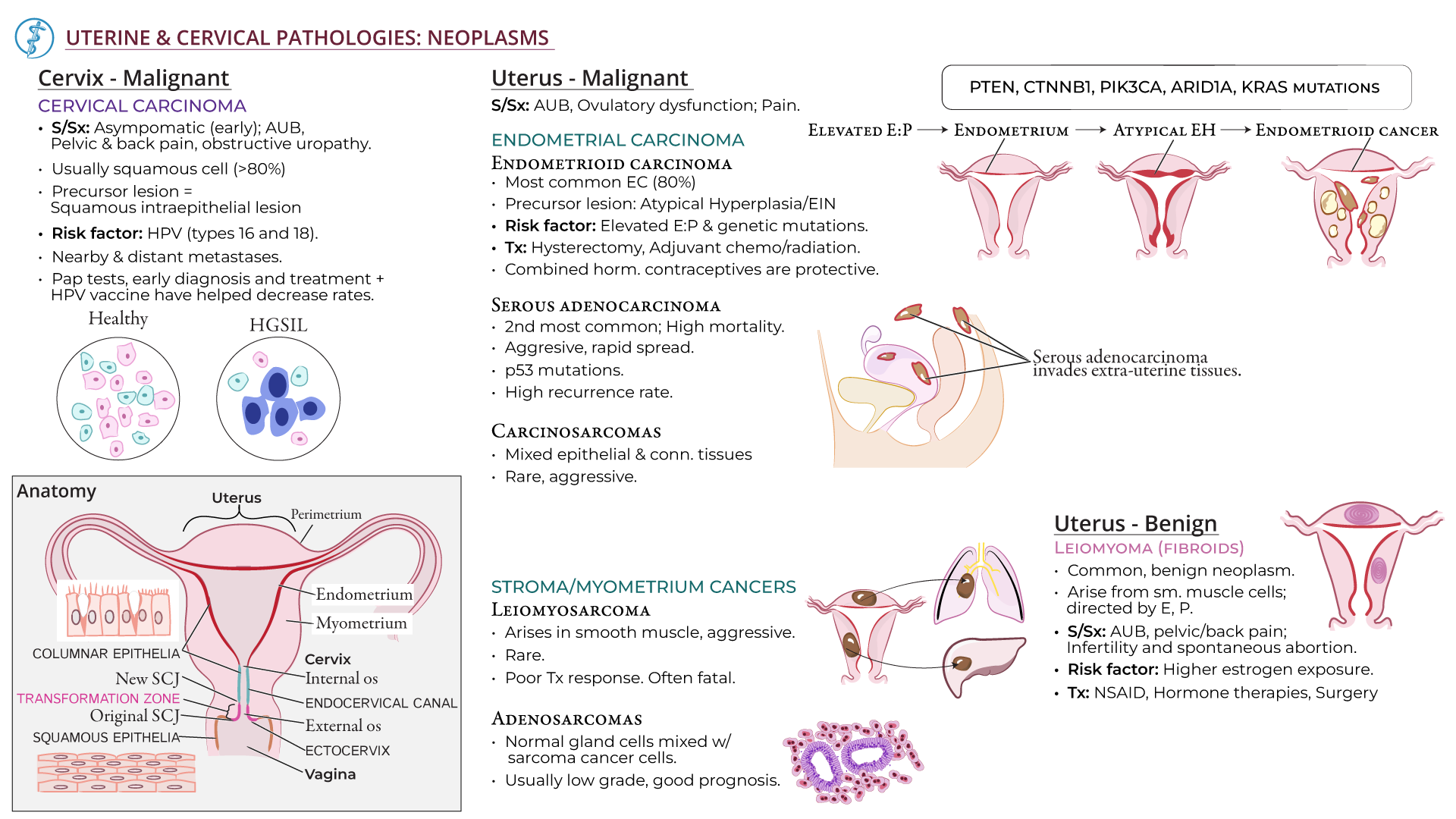
– Abnormal uterine bleeding refers to heavy or unusual bleeding from the uterus.
– Symptoms include vaginal bleeding between periods and extremely heavy bleeding during periods.
– Abnormal uterine bleeding can be caused by hormonal imbalances, pregnancy, polycystic ovary syndrome (PCOS), growths in the uterus (polyps or fibroids), infection, liver/kidney/thyroid disease, bleeding disorder, or cancer of the uterus/cervix.
– In teenagers and young adults, common causes include pregnancy, certain birth control methods, and hormonal imbalances.
– In the 40s and early 50s, abnormal uterine bleeding can be caused by a lack of ovulation, thickening of the uterine lining, or uterine cancer.
– Hormone replacement therapy is a common cause of uterine bleeding after menopause. There are various causes of abnormal uterine bleeding, including endometrial and uterine cancer. It is more common in older individuals. Other problems can also cause bleeding after menopause. It is important to consult a doctor if experiencing bleeding after menopause. Diagnosis may involve pregnancy tests, blood tests, ultrasound exams, endometrial biopsies, and hysteroscopy. Most causes of abnormal uterine bleeding are not preventable, but maintaining a healthy weight can help in some cases. Treatment options include birth control pills and intrauterine devices.
– One type of hormonal birth control, known as intrauterine devices (IUDs), can cause abnormal bleeding.
– A dilation and curettage (D&C) procedure involves stretching the cervix and using a surgical tool to scrape away the lining of the uterus. This procedure can be used to both diagnose and treat abnormal bleeding.
– Hysterectomy, the surgical removal of the uterus, stops menstrual bleeding and prevents pregnancy. It is a major surgery that requires general anesthesia and a hospital stay.
– Endometrial ablation is a surgical procedure that destroys the lining of the uterus but does not remove the uterus itself. It can often stop menstrual bleeding.
– Living with abnormal uterine bleeding can have a negative impact on daily life, causing anxiety and limiting activities.
– Ibuprofen can be taken during periods to help reduce pain and cramping.
– It is important to ensure adequate iron intake to prevent anemia.
– Questions to ask a doctor include the likely cause of abnormal bleeding, the seriousness of the condition, recommended treatment options, and the impact on future pregnancy chances.
– Doctors can determine if a woman has endometrial hyperplasia through medical history, symptoms, physical exam, and diagnostic tests.
– Medical history includes asking about irregular menstrual bleeding, menstrual history, pregnancy history, and medication usage.
– A pelvic exam may be normal as endometrial hyperplasia doesn’t cause physical changes to the reproductive system.
– Additional tests may be recommended, such as a transvaginal ultrasound to check the thickness of the uterine lining.
– If the uterine lining is too thick, a biopsy may be offered to diagnose the condition.
– In some cases, a procedure called dilation and curettage (D&C) and hysteroscopy may be performed.
– Results of the biopsy may show normal, abnormal non-cancerous, abnormal precancerous, or abnormal cancerous uterine lining cells.
– Abnormal findings that are non-cancerous and precancerous indicate endometrial hyperplasia.
– Granulosa-theca cell tumors (GCTs) are tumors of low malignant potential.
– Approximately 90% of GCTs are at stage I at the time of diagnosis.
– The 10-year survival rate for stage I tumors in adults is 90-96%.
– GCTs of more advanced stages are associated with 5- and 10-year survival rates of 33-44%.
– The overall 5-year survival rates for patients with adult-type granulosa cell tumors (AGCTs) or juvenile-type granulosa cell tumors (JGCTs) are 90% and 95-97%, respectively.
– The 10-year survival rate for AGCTs is approximately 76%.
– Recurrence rate for AGCTs is 43% in stage I-III patients observed over 10 years.
– Average recurrence for AGCTs is approximately 5 years after treatment, with more than half occurring more than 5 years after primary treatment.
– Mean survival after AGCT recurrence is 5 years.
– The 10-year overall survival after an AGCT recurrence is in the 50-60% range.
– JGCTs recur much sooner, with more than 90% of recurrences occurring in the first 2 years.
– Tumor stage at the time of initial surgery is the most important prognostic variable.
– Other factors associated with a poorer prognosis include high mitotic rates, moderate-to-severe atypia, preoperative spontaneous rupture of the capsule, and tumors larger than 15 cm.
– True thecomas have a 5-year survival rate of nearly 100%.
– 10% of GCTs occur during pregnancy, but this does not affect prognosis.
– AGCTs and JGCTs have very good cure rates due to early diagnosis.
– More than 90% of AGCTs and JGCTs are diagnosed before spread outside the ovary.
– Advanced-stage granulosa-stromal cell tumors (AGCTs) have a 25-50% 5-year survival rate.
– AGCTs can recur as late as 37 years after diagnosis.
– Mean survival after recurrence is 5 years.
– Approximately 20% of patients diagnosed with GCTs die from the disease.
– Morbidity is primarily due to endocrine manifestations of the disease.
– Removal of the tumor often regresses physical changes caused by high estrogen levels.
– Some patients may present with symptoms of androgen excess, which may partially regress over time.
– Unopposed estrogen production by these tumors can cause stimulation of the endometrium.
– 30-50% of patients develop endometrial hyperplasia and 8-33% have endometrial adenocarcinoma.
– Patients may be at an increased risk for breast cancer, although a direct correlation is difficult to prove.
– 10-15% of cases may have acute abdominal symptoms due to rupture, hemorrhage, or torsion.
– Adverse effects from chemotherapy are expected but generally well tolerated.
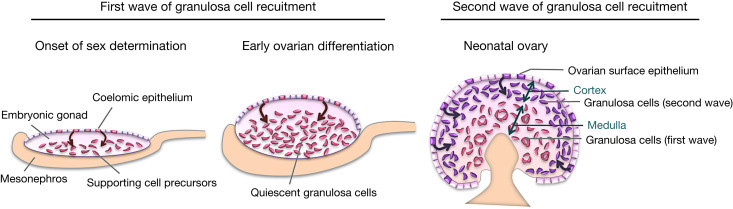
– Granulosa cell tumors (GCTs) are a type of ovarian tumor and the most common type of sex cord-stromal tumor in people assigned female at birth.
– Most GCTs are malignant (cancerous), but they tend to grow slowly and are often diagnosed in early stages with good treatment outcomes.
– Adult GCTs are more common, with about 95% of diagnoses in mature adult women.
– Juvenile GCTs occur in individuals under 30 and have a higher likelihood of recurring within a few years and being more aggressive if diagnosed after spreading outside the ovary.
– Leopold’s maneuvers are a common way to determine the position of a fetus in the uterus.
– They consist of four distinct actions and are important for assessing the potential complications during delivery.
– The skill of the examiner is crucial in correctly determining the fetal position.
– The maneuvers may be difficult to perform on obese women and those with polyhydramnios.
– The woman should be in a relaxed position and have recently emptied her bladder.
– The first maneuver involves palpating the upper abdomen to assess the size, consistency, shape, and mobility of the fetus.
– The second maneuver involves determining the location of the fetal back by palpating the abdomen with deep pressure.
– The third maneuver involves assessing the pelvic grip or Pawlik’s grip.
– The fourth maneuver involves determining the fetal descent and flexion.
– These maneuvers allow healthcare professionals to determine the baby’s size and placement in the uterus, as well as make a birth weight estimate.
– Leopold’s maneuvers should only be performed by trained medical professionals.
– They can help plan for a safe delivery and assess fetal weight and amniotic fluid volume.
– Leopold’s maneuvers are low-cost, non-invasive methods used to determine the position and estimated weight of a baby before birth.
– Leopold’s maneuvers do not require expensive equipment like an ultrasound.
– The ideal position for vaginal delivery is when the baby is head-down, facing the mother’s back, with their chin tucked to their chest.
– Most babies settle into this position between the 32nd and 36th week of pregnancy.
– Around 96% of babies are born in the cephalic position (head-down).
– The cephalic posterior position (baby is head-down but facing out instead of towards the spine) may increase the chances of a painful and prolonged delivery.
– A breech position (baby’s bottom is facing downwards) can make delivery riskier and may require a C-section.
– There are three types of breech positions: Frank breech, footling breech, and complete breech.
– A transverse lie position (baby lying sideways across the uterus) can also require a C-section if the baby doesn’t change position.
– Leopold’s maneuvers can be used to estimate the weight of the baby, which helps healthcare providers plan for birth.
– A baby estimated to be 10 pounds or more might require a C-section birth.
– There are no known risks associated with Leopold’s maneuvers when performed by qualified medical professionals.
– Leopold’s maneuvers are not as accurate before the 36th week of pregnancy.
– A full bladder can make determining the baby’s position accurately difficult, so providers may ask the patient to empty their bladder before the procedure.
– Leopold’s maneuvers may not be used if the mother has experienced blunt force trauma from an accident.
– Genital trauma refers to trauma to the genitalia, including the genital tract.
– Limited scientific data and evidence exist on genital injuries resulting from sexual assault.
– Studies on genital injuries have primarily focused on collecting evidence for legal purposes rather than medical purposes.
– Methods of studying and documenting genital injuries have improved through the use of tissue staining dyes and colposcopy.
– Vaginal trauma can occur during consensual and non-consensual intercourse, making it difficult to determine the circumstances based solely on a physical examination.
– Women are three times more likely to have vaginal injuries and intercourse-related injuries from a forced assault compared to consensual sexual experiences.
– Vaginal lacerations during intercourse may require surgery, while victims of forced assault may need additional services such as police intervention and trauma counseling.
– There is limited research on minor injuries in women of different age groups that do not require surgery or treatment.
– Factors that can predispose women to vaginal injury during consensual sex include first sexual experience, pregnancy, vigorous penetration, vaginal atrophy and spasm, previous operation or radiation therapy, disproportionate genitalia, penile ornamentation, and congenital anomalies.
– The missionary position with legs tilted all the way back during vaginal intercourse can lead to deep penetration and rotation of the uterus, potentially causing vaginal rupture.
– Vaginal tearing can occur in rape victims due to lack of vaginal lengthening and lubrication.
– Vulvar trauma is more common in prepubertal children and can occur from normal activities or sexual assault.
– Vaginal trauma can occur from the insertion of sharp objects, causing penetrating trauma.
– Severe vaginal injuries may require immediate medical attention if bleeding does not stop.
– Episiotomies can cause vaginal trauma.
– Penile trauma can occur in various forms, such as abrasions from zipper injuries or fractures from sexual activity.
– Penile amputation is a rare but emergency urological condition, often resulting from self-mutilation, accidents, or other causes.
– Micro-surgical repair is the most effective treatment method for penile trauma.
– Testicular trauma can occur from blunt, penetrating, or degloving injuries, particularly during contact sports.
– Wearing athletic cups can provide protection against testicular trauma.
– Testicular trauma can cause severe pain, bruising, swelling, and potential infertility.
– Vaginal atrophy is thinning, drying, and inflammation of the vaginal walls
– It occurs when the body has less estrogen, typically after menopause
– Vaginal atrophy can make intercourse painful and lead to distressing urinary symptoms
– Doctors use the term “genitourinary syndrome of menopause (GSM)” to describe vaginal atrophy and its symptoms
– Pap smears can detect atypical squamous cells in the cervix.
– The presence of abnormal squamous cells does not necessarily mean cervical cancer.
– Other possible causes of atypical squamous cells include HPV infection, benign cellular changes, cervical cysts or polyps, and low hormone levels in menopausal or post-menopausal patients.
– Further testing, such as re-analyzing the cell sample for HPV or additional exams like cervical biopsies, endocervical sampling exams, and colposcopies, may be recommended after an atypical Pap smear result.
– Detection of cancerous squamous cells during a Pap smear requires prompt treatment.
– Early detection of cervical cancer allows for more treatment options.
– Moffitt Cancer Center offers comprehensive diagnostic tests and treatments for cervical cancer, backed by the latest research and clinical trials.
– If someone has recently received abnormal Pap smear results with atypical squamous cells, they can call or submit an online form to request an appointment with a gynecologic oncologist at Moffitt Cancer Center.
– Virtual visits may be available, but in-person examination and evaluation are typically necessary for treatment decisions.
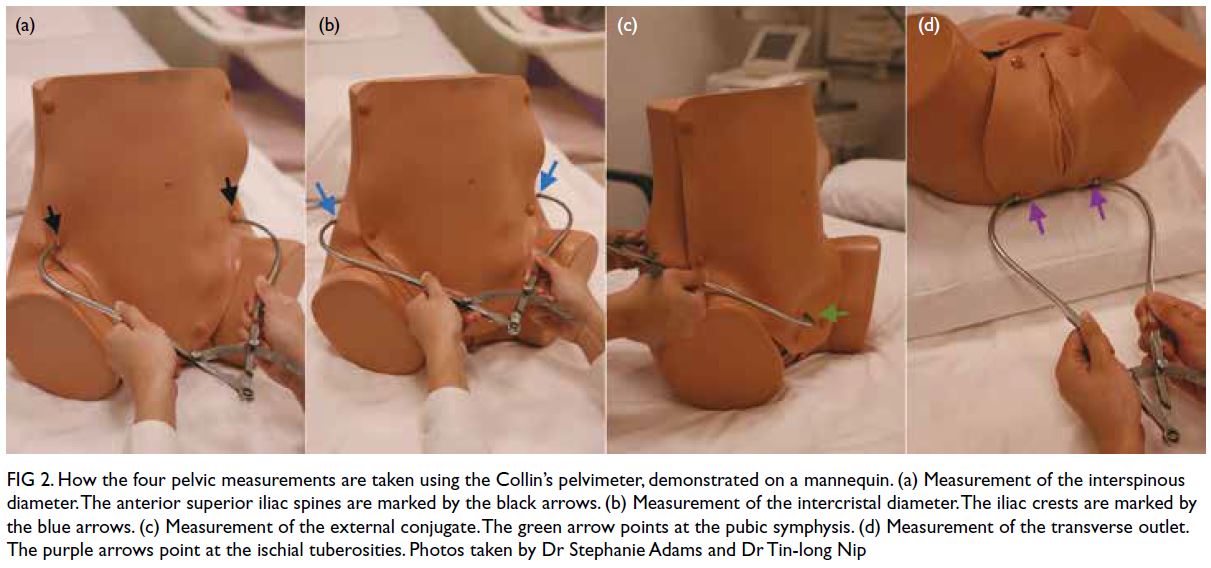
– external pelvimetry
– measuring pelvis size and shape
– predicting success of vaginal delivery
– third trimester of pregnancy
– calipers
– dimensions of the pelvis
– inlet, mid-pelvis, outlet
– limitations of external pelvimetry
– low sensitivity and specificity
– identifying cephalopelvic disproportion (CPD)
– false positive rate
– ultrasound pelvimetry
– clinical assessment
– more reliable methods
– non-invasive method
– evaluating maternal pelvic dimensions
– measuring pelvic landmarks
– calipers or tape measures
– adjunct to traditional methods
– internal pelvimetry
– determining suitability for vaginal delivery
– cesarean section
– limitations of external pelvimetry
– obesity
– fetal position
– pelvic soft tissue
– valuable information
– obstetric care