In the world of obstetrics, each birth is unique and brings its own set of challenges.
Imagine a scenario where a tiny human enters the world, presenting an unusual twist that leaves everyone in awe – a left mentoanterior face presentation.
This intriguing cephalic presentation, with its fully extended head, poses both excitement and concerns for medical professionals.
Today, we delve into the primary and secondary causes, the diagnostic procedures employed, the management techniques embraced, and the possible complications that may arise.
Join us on this extraordinary journey as we unravel the mysteries of face presentation, where negligence can lead to life-altering consequences.
left mentoanterior
Left mentoanterior refers to a cephalic presentation in which the baby’s head is completely extended and the face is presenting towards the birth canal.
This position occurs in about 1 in 300 labors.
Primary face presentation, which happens during pregnancy, may be caused by factors such as anencephaly, cord entanglement, foetal neck tumors, or muscular abnormalities.
Secondary face presentation can occur during labor and may be due to factors like a contracted pelvis or abnormal positions.
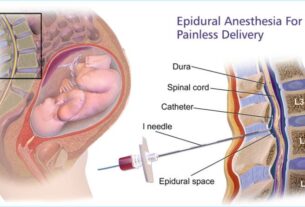
Diagnosis can be challenging but can be confirmed through ultrasound or X-ray during pregnancy, or through vaginal examination during labor, which shows identifying features of the face.
The mechanism of labor in left mentoanterior position involves descent, and spontaneous delivery usually occurs during the second stage of labor.
Forceps delivery, episiotomy, or caesarean section may be indicated in prolonged labor or if there are complications.
It is important to closely monitor the baby’s heart rate and avoid certain interventions that can put the baby at risk.
If medical negligence leads to injury, it can be considered a case of medical malpractice.
Key Points:
- Left mentoanterior is a cephalic presentation with the baby’s head extended and the face towards the birth canal.
- It occurs in about 1 in 300 labors.
- Primary face presentation can be caused by anencephaly, cord entanglement, foetal neck tumors, or muscular abnormalities.
- Secondary face presentation can occur during labor due to a contracted pelvis or abnormal positions.
- Diagnosis can be confirmed through ultrasound, X-ray, or vaginal examination.
- Delivery in left mentoanterior position usually occurs during the second stage of labor, with forceps delivery or caesarean section being indicated in prolonged labor or complications.
left mentoanterior – Watch Video
💡
Pro Tips:
1. The term “left mentoanterior” is commonly used in obstetrics to describe the position of the baby’s head during childbirth, where the chin is pointing towards the mother’s left thigh.
2. The left mentoanterior position is considered the most favorable fetal position for a vaginal birth, as it allows for an easier passage through the birth canal compared to other positions.
3. Research has found that babies in the left mentoanterior position may have a lower risk of umbilical cord compression during labor, leading to fewer complications during delivery.
4. During pregnancy, mothers may be advised to practice certain exercises and positions to encourage the baby to turn into a left mentoanterior position, promoting an optimal birthing experience.
5. In rare cases, if the baby remains in a right mentoanterior position (opposing the left mentoanterior), it can increase the risk of prolonged labor and potential complications, often requiring medical intervention.
Incidence Of Face Presentation In Labours
Face presentation is a relatively rare occurrence in childbirth, with an incidence of about 1 in 300 labors. It is characterized by the baby’s head being completely extended, resulting in the face being the presenting part during delivery. Unlike normal cephalic presentations where the baby’s head is flexed, in face presentation, the head is in an extended position, causing the face to enter the birth canal first.
- Incidence of face presentation is approximately 1 in 300 labors.
- Face presentation occurs when the baby’s head is completely extended.
- The face is the presenting part during delivery.
- Unlike normal cephalic presentations, the head is in an extended position in face presentation.
- Face presentation can result in challenges during delivery due to the position of the baby’s head.
“Face presentation is characterized by the baby’s head being completely extended, resulting in the face being the presenting part during delivery.”
Causes Of Primary And Secondary Face Presentation
Primary face presentation occurs during pregnancy and can be caused by various factors, including:
- Anencephaly: a severe neural tube defect
- Nuchal cord: loops of the umbilical cord around the neck
- Fetal neck tumors
- Hypertonicity of the neck muscles
- Dolicocephaly: an elongated head shape
- A dead or premature fetus
- Idiopathic causes where no specific reason can be identified
On the other hand, secondary face presentation occurs during labor and can be attributed to different factors, such as:
- A contracted pelvis
- A pendulous abdomen: a downwardly hanging belly
- Marked lateral obliquity of the uterus: a tilted or angled womb
- Further deflexion of the brow or occipito-posterior positions: abnormal head positions
- Other malpresentations such as polyhydramnios: excessive amniotic fluid and placenta previa: abnormal positioning of the placenta.
Common Positions Of Face Presentation
The left mento-anterior (LMA) and right mento-anterior (RMA) positions are the most commonly observed orientations in face presentations. In these positions, the baby’s head is positioned with the chin (mentum) facing forward and either to the left or to the right side of the mother’s pelvis. It is important to note that other positions, such as the mento-posterior (chin facing the mother’s back), may also occur but are less frequent.
To summarize:
- The LMA and RMA positions are frequently seen in face presentations.
- These positions involve the baby’s head with the chin facing either left or right.
- The mento-posterior position, with the chin facing the mother’s back, is less common.
“The left mento-anterior (LMA) and right mento-anterior (RMA) positions are more commonly observed in face presentations.”
Diagnosis Of Face Presentation During Pregnancy
Diagnosing face presentation during pregnancy can be challenging. However, there are certain signs that may suggest this presentation, including:
- Difficulty feeling the baby’s back
- More prominent sensation of the baby’s limbs in the mento-anterior position
Confirming the diagnosis typically requires the use of additional tools such as ultrasound or X-ray imaging.
Note: Diagnosing face presentation in pregnancy can be challenging. Certain signs, such as difficulty feeling the baby’s back and a more prominent sensation of the baby’s limbs in the mento-anterior position, may suggest this presentation. Confirming the diagnosis usually requires the use of additional tools like ultrasound or X-ray imaging.
Diagnosis Of Face Presentation During Labour
The diagnosis of face presentation during labor is primarily done through a vaginal examination. This examination allows healthcare professionals to identify specific features of the baby’s face, including the supra-orbital ridges, malar processes, nose, mouth, and chin. By palpating these facial landmarks, a diagnosis of face presentation can be made.
Differentiating Face Presentation From Breech Presentation
Late in labor, the face in a face presentation may become edematous or swollen, which can lead to potential misdiagnosis as a breech presentation (where the baby’s buttocks or feet enter the birth canal first). However, there are several differentiating factors that can help distinguish between the two. These include:
- The formation of a triangular shape with the fetal mouth and malar processes as apexes.
- The presence of the anus on the same line as the ischial tuberosities (bony points in the pelvis).
- The feeling of a hard gum through the mouth.
- The absence of a hard object through the anus.
Mechanism Of Labour In Mento-Anterior Position
In the mento-anterior position, the mechanism of labor involves the baby’s descent through the birth canal in preparation for delivery. The engagement of the baby occurs when the submento-bregmatic diameter, measuring approximately 9.5 cm, passes through the maternal pelvis. As labor progresses, the submental region of the baby’s head hinges below the symphysis (central joint) of the pelvis, allowing for further descent. The submento-vertical diameter, measuring approximately 11.5 cm, is crucial as it determines whether the baby’s head can pass through the pelvic inlet. Only when the chin is below the level of the ischial spines (bony landmarks in the pelvis) and the face begins to distend the perineum does the biparietal diameter (the distance between the two sides of the baby’s head) pass the plane of the pelvic inlet.
Management Of Face Presentation During Labour
The management of face presentation during labor involves several considerations. Key points to consider are:
-
Exclude fetal anomalies and contracted pelvis: Further investigations and assessments should be conducted to rule out any potential fetal anomalies or contracted pelvis.
-
Spontaneous delivery: In the second stage of labor, it is common for the baby to be in the mento-anterior position, which allows for spontaneous delivery.
-
Prolonged second stage of labor: If the second stage of labor becomes prolonged, interventions such as forceps delivery and episiotomy (a surgical incision to widen the birth canal) may be necessary.
-
Mento-posterior position: In cases of mento-posterior position, healthcare providers should wait for a long anterior rotation of approximately 3/8 circle before proceeding with delivery.
-
Administration of oxytocin: If necessary, oxytocin may be administered to overcome inertia (lack of progress) during this period, as long as there are no contraindications.
-
Caesarean section: If long anterior rotation fails or there is evidence of fetal or maternal distress, a caesarean section is the safest option.
-
Avoid hazardous methods: Alternative methods such as manual rotation and forceps extraction or rotation and extraction by Kielland forceps are considered hazardous and are not commonly used.
-
Fetus found to be deceased: In instances when the fetus is found to be deceased, a craniotomy (surgical procedure to collapse the baby’s skull) may be performed to facilitate delivery.
-
Overall, the management of face presentation during labor requires careful evaluation and consideration of the specific circumstances.
Complications Of Face Presentation
Face presentation is associated with a higher risk of complications compared to normal cephalic presentations. Some of the potential complications include prolonged labor, facial trauma, facial edema (swelling), skull molding (temporary reshaping of the baby’s skull), respiratory distress, spinal cord injury, abnormal fetal heart rate patterns, and low Apgar scores (a scoring system used to assess newborns’ overall health). It is crucial to closely monitor the fetal heart rate throughout labor to promptly identify any abnormalities and provide appropriate interventions when necessary.
Legal Considerations And Medical Malpractice Involving Face Presentation
In cases involving face presentation, it is crucial for healthcare professionals to obtain informed consent from the mother. Failure to do so can be considered negligence and may have legal consequences.
Additionally, it is important to be aware that the use of forceps and oxytocin during labor to manage complications associated with face presentation can pose risks to the baby. For instance, forceps delivery can potentially cause head injuries. Likewise, the administration of oxytocin can result in oxygen deprivation for the baby due to the occurrence of strong contractions. In light of these potential complications, mothers should be offered the option of a caesarean section if complications arise.
In the unfortunate event that negligent practices during a face presentation delivery lead to injury for the baby, it may be considered a case of medical malpractice. In such situations, seeking legal advice becomes crucial. Legal consultancies like ABC Law Centers specialize in birth injury cases and provide free consultations to individuals seeking assistance in these matters.
💡
You may need to know these questions about left mentoanterior
What is left mento anterior?
When the mentum presents in the left anterior quadrant of the maternal pelvis, it is referred to as left mentum anterior (LMA). This positioning can have significant implications during childbirth. The LMA position may affect the progress of labor, the engagement of the fetal head, and the overall ease of delivery. Obstetricians closely monitor the presentation of the mentum to ensure a safe and successful birth for both the mother and the baby.
What is the difference between Mentoanterior and Mentoposterior?
The main difference between Mentoanterior and Mentoposterior positions lies in the location of the chin in relation to the limbs and occiput. In Mentoanterior position, the limbs are felt more pronounced and the chin can be observed on the same side as the limbs, forming a horseshoe-shaped rim. On the other hand, in Mentoposterior position, a groove may be felt between the occiput and the back, especially after the membranes have ruptured. This distinction helps in identifying the positioning of the baby and providing appropriate medical assistance during childbirth.
What is the difference between Mento anterior and Mento posterior?
The difference between Mento anterior and Mento posterior lies in the orientation of the baby’s chin in relation to the mother. Mento anterior position occurs when the chin is facing the front of the mother, making it the leading part of the face during delivery. Babies in this position are commonly delivered vaginally, but there may be instances where a C-section is required. On the other hand, Mento posterior (MP) position refers to the chin facing the mother’s back. This orientation can present certain challenges during childbirth and may increase the likelihood of a cesarean delivery.
What is the RMA position of the fetus?
The fetus in the RMA position refers to the Right Mentum Anterior position, which means that the mentum (the chin) is on the right side of the pelvis, with the back closest to the mother’s belly. This positioning of the fetus can have certain implications during pregnancy and childbirth, as it may affect the delivery process. Obstetricians closely monitor the RMA position to ensure the well-being of both the mother and the baby, employing appropriate techniques and interventions if necessary.
Reference source
https://www.gfmer.ch/Obstetrics_simplified/face_presentation.htm
https://www.abclawcenters.com/practice-areas/prenatal-birth-injuries/abnormal-position-or-presentation/face-presentation/
https://twincitiesmidwifery.com/left-occiput-what/
https://www.gfmer.ch/Obstetrics_simplified/face_presentation.htm