Are you curious about how your birthing position can affect the rotation of your baby’s head during labor?
Imagine a groundbreaking study that explores the potential benefits of the hands and knees position compared to traditional expectant management.
Dive into the fascinating world of left occipitoposterior research and uncover the secrets that may revolutionize childbirth.
left occipitoposterior
The study aims to evaluate the effects of different positions on the outcome of occipitoposterior (OP) position during labor.
The study will compare the hands and knees position with expectant management (no intervention).
It will include nulliparous and multiparous women during the first stage of labor with a cervical dilatation between 2 to 9 cm, a singleton pregnancy at term, and an OP position diagnosed by ultrasound.
The study interventions involve women in the hands and knees position group choosing one of six positions.
The primary outcome measure is fetal head in anterior position.
Data analysis will be performed using statistical tests, and a sample size of 438 women is needed to show a statistically significant difference in the incidence of the main outcome measure.
The study protocol has been approved by the institutional ethics committee, and safety considerations for mothers and fetuses will be closely monitored.
The study aims to be completed in June 2014.
Key Points:
- Study aims to evaluate the effects of different positions on outcomes of occipitoposterior (OP) position during labor
- Hands and knees position will be compared with expectant management (no intervention)
- Study includes nulliparous and multiparous women in first stage of labor, with cervical dilation between 2 to 9 cm and an OP position diagnosed by ultrasound
- Women in hands and knees position group will choose one of six positions as intervention
- Primary outcome measure is fetal head in anterior position
- Data analysis will be performed using statistical tests, with a sample size of 438 women needed to show a significant difference in the main outcome measure incidence
left occipitoposterior – Watch Video
💡
Pro Tips:
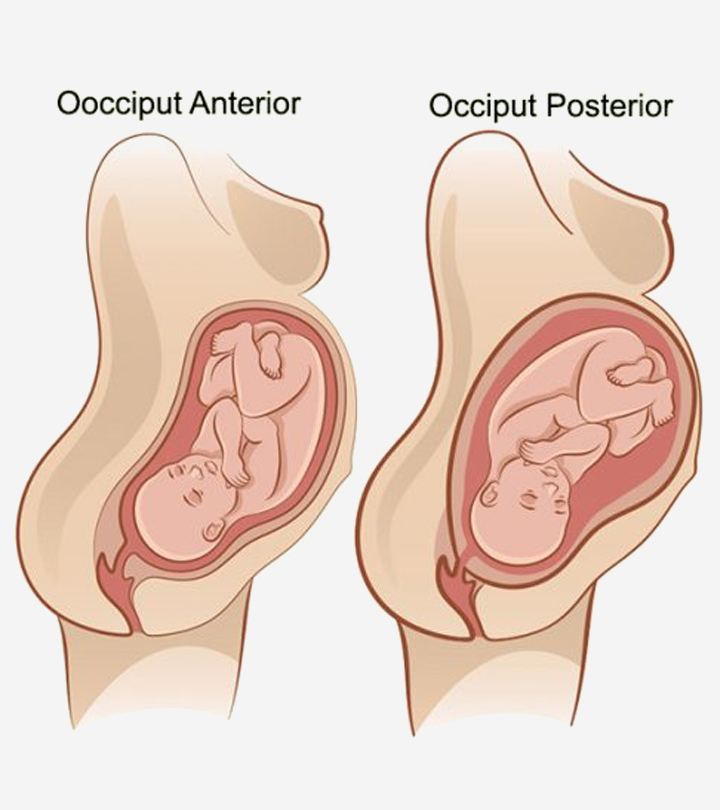
1. The left occipitoposterior (LOP) position in obstetrics refers to the position of the baby’s head in the mother’s pelvis during labor, with the baby’s occiput (back of the head) facing towards the mother’s left side.
2. LOP is considered one of the more challenging positions for birth, as it can lead to a longer and more difficult labor for both mother and baby.
3. In some cases, a baby in the LOP position may rotate spontaneously during labor and end up in the more favorable occipitoanterior (OA) position, which is associated with a smoother and easier delivery.
4. The LOP position can cause intense back pain for the mother during labor due to the baby’s head pressing against the lower back.
5. Certain positions and exercises, such as pelvic tilts and hands-and-knees positions, can help encourage the baby in the LOP position to rotate to a more favorable position during labor.
Objective Of The Study
The objective of this randomised clinical trial is to evaluate the effects of different positions on the outcome of occipitoposterior (OP) positions during labor. The study aims to compare the hands and knees position with expectant management (no intervention) and assess the effectiveness of various positions on fetal head rotation, comfort of maternal positions, pain perception, duration of labor stages, mode of delivery, perineal status, and neonate outcomes. The primary outcome measure is fetal head in anterior position. By examining the impact of different positions, the study seeks to provide valuable insights and potentially improve the management of OP positions during labor.
Inclusion Criteria For Participants
The study will include nulliparous and multiparous women during the first stage of labor with a cervical dilatation between 2 to 9 cm, a singleton pregnancy at term (≥ 37 weeks’ gestation), and an OP position diagnosed by ultrasound. This specific population of participants was chosen to ensure consistency and comparability in the study findings. By focusing on women experiencing labor with OP positions, the study can provide specific recommendations for this particular situation.
- Nulliparous and multiparous women
- Cervical dilatation between 2 to 9 cm
- Singleton pregnancy at term (≥ 37 weeks’ gestation)
- OP position diagnosed by ultrasound
“The specific population of participants in this study includes nulliparous and multiparous women during the first stage of labor, with a cervical dilatation between 2 to 9 cm, a singleton pregnancy at term (≥ 37 weeks’ gestation), and an OP position diagnosed by ultrasound.”
Exclusion Criteria For Participants
Certain groups of women will be excluded from the study to maintain the integrity of the results. The following women will not be included in the study:
- Women under 18 years old,
- Women with limited understanding of French, and
- Women who have attempted hands and knees positions previously during labor.
These exclusion criteria are in place to eliminate potential confounding factors that could impact the study outcomes. By excluding these groups, the researchers can focus on the effects of different positions on women who have not previously tried the hands and knees position.
Study Design And Randomisation
The study will be a randomised clinical trial, employing a web-based system for randomisation. The ratio for hands and knees position versus expectant management is 1:1, ensuring a balanced representation of participants in both groups. Randomisation is essential to minimise bias and ensure that the results accurately reflect the effects of different positions on the outcome of OP position during labor. The use of a web-based system provides an efficient and secure method for randomisation, ensuring the integrity of the study design.
Interventions In The Hands And Knees Position Group
Participants assigned to the hands and knees position group will have the opportunity to choose one of six positions described by Dr. de Gasquet. These positions are carefully designed to maximize comfort and encourage optimal fetal head rotation.
The study interventions involve observing three important points:
- Resting on the knees and hands if necessary
- Thrusting the abdomen forward
- Keeping the back stretched
Participants may use a pillow for added comfort, and they can choose to place their abdomen on a cushion or leave it unsupported. These interventions aim to provide a range of options so that participants can find a position that suits their individual needs.
“The hands and knees position group offers participants the chance to select from six positions recommended by Dr. de Gasquet. These positions are specifically tailored to enhance comfort and facilitate the rotation of the fetal head. The interventions involve adhering to three key principles:“
- Resting on the knees and hands if needed
- Thrusting the abdomen forward
- Keeping the back stretched
“In order to ensure greater comfort, participants have the option to use a pillow and decide whether to support their abdomen with a cushion or leave it unsupported. These interventions provide a variety of choices to suit each participant’s unique requirements.“
Important Points To Observe In The Fitted Positions
In the hands and knees position, there are six fitted positions that can be used. It is crucial for participants to observe three important points while assuming these positions.
First, participants should rest on their knees and hands if necessary to maintain a comfortable and stable position.
Second, they should thrust their abdomen forward, which helps create the optimal environment for fetal head rotation.
Finally, it is important to keep the back stretched to avoid any unnecessary strain or discomfort.
By paying attention to these important points, participants can ensure that they are adopting the positions correctly and maximising the potential benefits.
Management Of The Op Position By Midwives
All midwives in the delivery room have undergone training in managing the OP position using specific hand and knee positions. This training ensures that the midwives are equipped with the necessary skills and knowledge to provide appropriate support and guidance to participants in the hands and knees position group. With their expertise, the midwives can assist participants in assuming the correct positions and offer any necessary adjustments for comfort and optimal fetal head rotation.
The involvement of trained midwives contributes to the consistency and quality of care provided to participants throughout the study.
- Trained midwives offer support and guidance in managing the OP position
- Specific hand and knee positions are used for optimal fetal head rotation
- Midwives provide necessary adjustments for comfort during the hands and knees position
- Their expertise contributes to consistency and quality of care throughout the study
Expectant Management Arm And Usual Care
Participants assigned to the expectant management arm will receive usual care during labor. After one hour, they will have the option to adopt a hands and knees position if desired. The position of the woman during this hour will be recorded for analysis.
The expectant management arm allows for a comparison between participants who receive no intervention and those who actively choose to assume the hands and knees position. By including this arm, the study can assess the benefits of immediate hands and knees positioning versus waiting for one hour before adopting the position.
To summarize:
- Participants in the expectant management arm receive usual care during labor.
- After one hour, they can choose to adopt a hands and knees position.
- The woman’s position during this hour is recorded for analysis.
Outcome Measures And Data Collection
Several outcome measures will be assessed in this study. The primary outcome measure is the fetal head in the anterior position. Other secondary outcome measures include:
- Comfort of maternal positions
- Pain perception
- Duration of labor stages
- Mode of delivery
- Perineal status
- Neonate outcomes
To collect these data, participants in both groups will complete a questionnaire on perceived pain and comfort. Fetal head position will be verified one hour after randomisation or at delivery.
The study design ensures a comprehensive evaluation of the effects of different positions on both maternal and neonatal outcomes.
Study Timeline And Ethical Considerations
The study is expected to be completed in June 2014.
-
A sample size of 438 women is needed to show a statistically significant difference in the incidence of the primary outcome measure.
-
The study estimates that around 300 eligible women per year will be proposed for study entry, and the required sample size could be reached in approximately 35 months.
The study protocol has been approved by the institutional ethics committee, ensuring that the study is conducted ethically and with consideration for the safety and well-being of mothers and fetuses.
The study also guarantees that women have the right to withdraw consent without impacting the quality of care or staff attitude.
Data will be kept confidential, and participants will be identified with a number to ensure privacy.
The study results will be reported anonymously, further protecting the participants’ identities.
–
💡
You may need to know these questions about left occipitoposterior
What does left Occipito posterior position mean?
In a left Occipito posterior position, the baby’s head is positioned downwards, but it is facing towards the mother’s front rather than her back. This position, although safe for delivery, can present some challenges during childbirth. The baby may encounter difficulty passing through the pelvis due to the alignment, potentially leading to a more prolonged or difficult labor. Special techniques and positions may be employed to assist the baby in navigating through the pelvis and facilitate a smoother delivery.
What are the complications of left occiput posterior?
The left occiput posterior position can result in complications during childbirth. Due to the baby’s position, it can cause intense back pain, commonly known as back labor, making the birthing process more uncomfortable for the mother. Additionally, this presentation may lead to slower progress in labor, potentially prolonging the overall duration of childbirth.
How does occiput posterior affect labor?
Occiput posterior (OP) position can significantly impact labor. Women with an OP position often experience more interventions during labor, such as induction and augmentation to progress labor. Additionally, the first and second stages of labor tend to be longer, leading to potential complications such as chorioamnionitis, post-partum hemorrhage, and perineal tears. These women may also be at a higher risk of developing infections such as wound infection and endometritis. Managing and addressing the complications associated with the occiput posterior position is crucial to ensure a safe and healthy labor and delivery experience.
What causes Occipitoposterior position?
The occipitoposterior position is primarily caused by the natural adaptation of the fetal head to the mother’s pelvis, which may have a narrow fore pelvis but an ample anteroposterior diameter. This can be considered a normal physiological response. As the baby moves into the birth canal, the head adjusts to fit in the optimal position for birth. In some cases, this adjustment leads to the occiput (back of the head) facing towards the mother’s back, resulting in the occipitoposterior position.
Reference source
https://www.in.pampers.com/pregnancy/pregnancy-symptoms/article/occiput-posterior-and-its-effect-on-labor
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4436169/
https://www.sciencedirect.com/science/article/pii/S0002937841902612
https://www.verywellfamily.com/fetal-positions-for-labor-and-birth-2759020