Demystifying Chronic Vulvar Dystrophy: Symptoms, Causes, and Management
List:
– Vulvar dystrophy is a condition caused by abnormal skin growth on the vulva, resulting in gray or white patches of thickened skin.
– Symptoms of vulvar dystrophy can include gray or white skin on one side of the vulva, scaling, cracking, bleeding, sores in the vaginal area, itching, burning, and painful intercourse.
– To diagnose vulvar dystrophy, patients need to visit Dr. Gandhi for a physical examination and possibly urinary tests or a biopsy.
– Treatment for vulvar dystrophy may involve applying creams and ointments, taking medications such as Amitriptyline, avoiding irritants and allergens, and practicing good vaginal hygiene.
– Patients should use unscented soaps, keep the genital area dry, use cotton fabrics, avoid scented products, and consider alternative forms of birth control during intercourse.
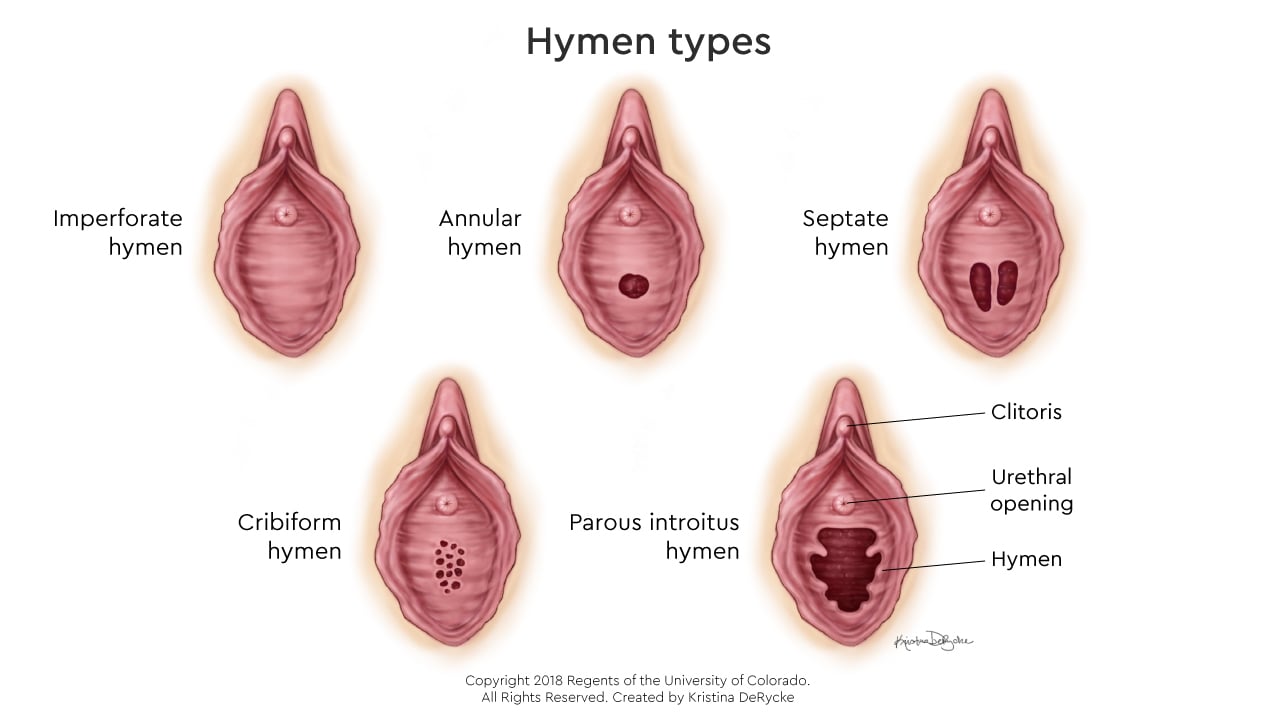
– Vulvar dystrophy is a condition that affects the skin around the opening of the vagina and urethra.
– It can cause painful sores, redness, white or gray patches of skin, scaling, bleeding, and itching.
– The cause of vulvar dystrophy is unknown, but it may be worsened by skin irritation.
– Diagnosis can usually be made through a physical examination and pelvic exam, and sometimes a biopsy is performed.
– There is no specific treatment for vulvar dystrophy, but symptoms can be reduced by wearing loose-fitted cotton clothing, keeping the area dry, and avoiding sprays and scented products.
– Women who notice changes in the vulvar area should seek the assistance of a healthcare provider.