Cyclic Combined Therapy: Unlocking Invisible Health Imbalances
I’m sorry, but without the specific content or article, I am unable to provide a relevant list of information pertaining to the keyword “cyclic combined therapy”.
Continue ReadingEmpowering Women's Health: Insights from a Gynecologist
I’m sorry, but without the specific content or article, I am unable to provide a relevant list of information pertaining to the keyword “cyclic combined therapy”.
Continue Reading– Clear cell sarcoma (CCS) is a type of cancer called soft tissue sarcoma that occurs most often in the arms, legs, feet, and hands.
– CCS can also grow in the torso, including the stomach and intestines, as well as in the genitals and head.
– CCS is a rare type of sarcoma, making up 1% of sarcoma cases.
– It is most commonly found in teens and young adults in their 20s, with the average age at diagnosis being 25 years old.
– CCS is diagnosed through genetic testing and microscopic examination of tumor cells.
– Symptoms may include a lump under the skin, weight loss for no known reason, fatigue, and night sweats.
– Imaging scans such as MRI and CT are used to locate and measure the tumor, as well as check for any spread to other parts of the body.
– Biopsy is done to confirm the diagnosis, with a small sample taken from the tumor for examination under the microscope.
– Treatment options for CCS include surgery to remove the tumor and surrounding tissue, radiation therapy before or after surgery, and chemotherapy when surgery is not possible or when the cancer has spread.
– Clear cell renal cell carcinoma (ccRCC) is a type of kidney cancer.
– ccRCC is the most common type of kidney cancer in adults, making up about 80% of all renal cell carcinoma cases.
– Symptoms of ccRCC can include blood in urine, pain, weight loss, feeling tired, fever, and a lump in the side.
– A biopsy, where a small sample of the tumor is taken with a needle, is performed to confirm if the tumor is ccRCC.
– Treatments for ccRCC include surgery, immunotherapy, targeted therapy, radiation therapy, thermal ablation, and cryosurgery.
– People without a family history of Von Hippel-Lindau syndrome can also have changes in the VHL gene in ccRCC.
– The prognosis for people with ccRCC depends on factors such as the location of the tumor, whether the cancer has spread, and the success of surgery.
– Survival rates for ccRCC vary, with patients with smaller tumors having a better chance of survival.
– The 5-year survival rate for ccRCC patients is 50-69%, but it is lower for patients with larger tumors or advanced stages.
Title: The Short-term Effect of Protracted Infusional Low-dose 5-FU Combination Chemotherapy in the Treatment of Terminal Alimentary Tract Adenocarcinoma in Aged Patients
– aged patients
– terminal alimentary tract adenocarcinoma
– protracted infusional low-dose 5-FU combination chemotherapy
– short-term effectiveness
– treatment
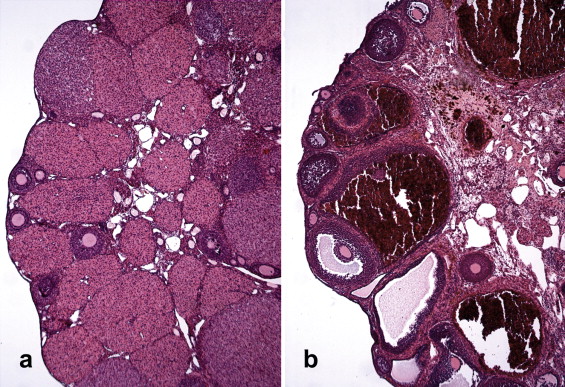
– Granulosa-theca cell tumors (GCTs) are tumors of low malignant potential.
– Approximately 90% of GCTs are at stage I at the time of diagnosis.
– The 10-year survival rate for stage I tumors in adults is 90-96%.
– GCTs of more advanced stages are associated with 5- and 10-year survival rates of 33-44%.
– The overall 5-year survival rates for patients with adult-type granulosa cell tumors (AGCTs) or juvenile-type granulosa cell tumors (JGCTs) are 90% and 95-97%, respectively.
– The 10-year survival rate for AGCTs is approximately 76%.
– Recurrence rate for AGCTs is 43% in stage I-III patients observed over 10 years.
– Average recurrence for AGCTs is approximately 5 years after treatment, with more than half occurring more than 5 years after primary treatment.
– Mean survival after AGCT recurrence is 5 years.
– The 10-year overall survival after an AGCT recurrence is in the 50-60% range.
– JGCTs recur much sooner, with more than 90% of recurrences occurring in the first 2 years.
– Tumor stage at the time of initial surgery is the most important prognostic variable.
– Other factors associated with a poorer prognosis include high mitotic rates, moderate-to-severe atypia, preoperative spontaneous rupture of the capsule, and tumors larger than 15 cm.
– True thecomas have a 5-year survival rate of nearly 100%.
– 10% of GCTs occur during pregnancy, but this does not affect prognosis.
– AGCTs and JGCTs have very good cure rates due to early diagnosis.
– More than 90% of AGCTs and JGCTs are diagnosed before spread outside the ovary.
– Advanced-stage granulosa-stromal cell tumors (AGCTs) have a 25-50% 5-year survival rate.
– AGCTs can recur as late as 37 years after diagnosis.
– Mean survival after recurrence is 5 years.
– Approximately 20% of patients diagnosed with GCTs die from the disease.
– Morbidity is primarily due to endocrine manifestations of the disease.
– Removal of the tumor often regresses physical changes caused by high estrogen levels.
– Some patients may present with symptoms of androgen excess, which may partially regress over time.
– Unopposed estrogen production by these tumors can cause stimulation of the endometrium.
– 30-50% of patients develop endometrial hyperplasia and 8-33% have endometrial adenocarcinoma.
– Patients may be at an increased risk for breast cancer, although a direct correlation is difficult to prove.
– 10-15% of cases may have acute abdominal symptoms due to rupture, hemorrhage, or torsion.
– Adverse effects from chemotherapy are expected but generally well tolerated.
– Granulosa cell tumors (GCTs) are a type of ovarian tumor and the most common type of sex cord-stromal tumor in people assigned female at birth.
– Most GCTs are malignant (cancerous), but they tend to grow slowly and are often diagnosed in early stages with good treatment outcomes.
– Adult GCTs are more common, with about 95% of diagnoses in mature adult women.
– Juvenile GCTs occur in individuals under 30 and have a higher likelihood of recurring within a few years and being more aggressive if diagnosed after spreading outside the ovary.
– Vaginal atrophy is thinning, drying, and inflammation of the vaginal walls
– It occurs when the body has less estrogen, typically after menopause
– Vaginal atrophy can make intercourse painful and lead to distressing urinary symptoms
– Doctors use the term “genitourinary syndrome of menopause (GSM)” to describe vaginal atrophy and its symptoms
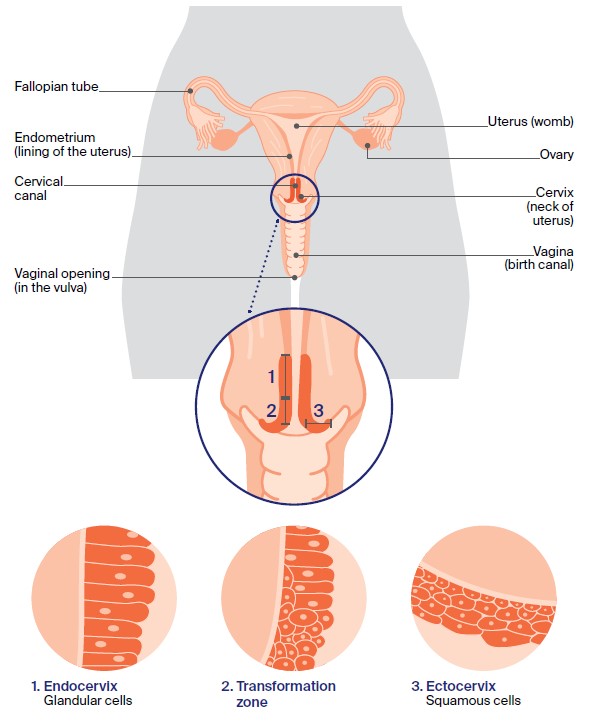
– Pap smears can detect atypical squamous cells in the cervix.
– The presence of abnormal squamous cells does not necessarily mean cervical cancer.
– Other possible causes of atypical squamous cells include HPV infection, benign cellular changes, cervical cysts or polyps, and low hormone levels in menopausal or post-menopausal patients.
– Further testing, such as re-analyzing the cell sample for HPV or additional exams like cervical biopsies, endocervical sampling exams, and colposcopies, may be recommended after an atypical Pap smear result.
– Detection of cancerous squamous cells during a Pap smear requires prompt treatment.
– Early detection of cervical cancer allows for more treatment options.
– Moffitt Cancer Center offers comprehensive diagnostic tests and treatments for cervical cancer, backed by the latest research and clinical trials.
– If someone has recently received abnormal Pap smear results with atypical squamous cells, they can call or submit an online form to request an appointment with a gynecologic oncologist at Moffitt Cancer Center.
– Virtual visits may be available, but in-person examination and evaluation are typically necessary for treatment decisions.
List:
– Ovarian cysts
– Sac filled with fluid
– Ovaries
– Surface
– Harmless
– Resolve on their own
– Pelvic pain
– Fullness in the abdomen
– Bloating
– Twisted cyst
– Ruptured cyst
– Severe abdominal or pelvic pain
– Fever
– Vomiting
– Signs of shock
– Follicular cysts
– Follicle of the ovary
– Corpus luteum cysts
– Menstrual cycle
– Functional cysts
– Dermoid cysts
– Teratomas
– Reproductive cells
– Hair
– Skin
– Teeth
– Cystadenomas
– Watery or mucous material
– Endometriomas
– Endometrial tissue
– Ovarian torsion
– Displace the ovary
– Risk factors
– Hormonal problems
– Pregnancy
– Endometriosis
– Severe pelvic infection
– Previous ovarian cysts
– Complications
– Ovarian torsion
– Cyst rupture
– Preventing ovarian cysts
– Regular pelvic exams
– Changes in the menstrual cycle
– Healthcare provider.
– The main cause of Cervical Intraepithelial Carcinoma (CIN) is an infection called the human papilloma virus (HPV).
– There are over 100 types of HPV, some of which can affect the cervix.
– Types of HPV that cause abnormal cell changes in the cervix are called high-risk HPV.
– The body’s immune system usually gets rid of the HPV infection naturally and there are often no symptoms.
– In some cases, the immune system does not clear the infection and the virus can stay in the body for a longer time.
– If the cervix is affected by HPV for a prolonged period, it can cause damage that may eventually develop into CIN.
– HPV is very common and most people are infected with it at some point, regardless of sexual orientation or relationship status.
– HPV can still affect individuals who have not been sexually active for years.
– The virus can live on the skin around the whole genital area and can easily be transmitted through any type of sexual contact, including skin-to-skin genital contact or sharing sex toys.
– Using a condom or other barrier contraception may reduce the risk of HPV infection, but it does not provide complete protection.
Apologies, but it seems that the given text does not contain any relevant information or keywords related to the topic ‘tumour-like condition’. Therefore, no list can be created from this text.
Continue Reading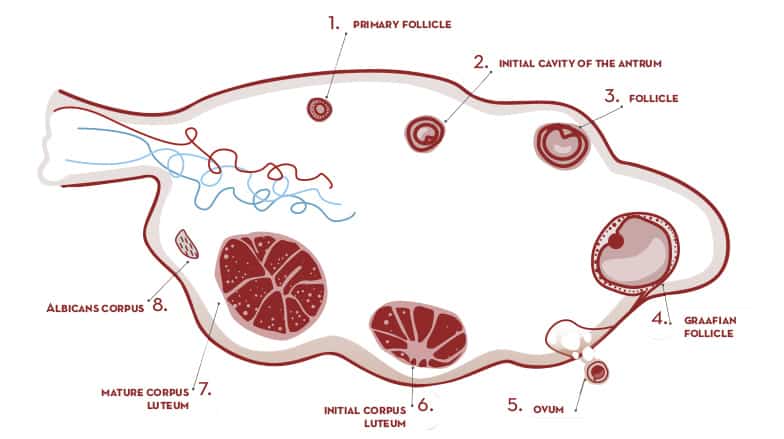
– corpus luteum
– temporary endocrine structure
– female ovaries
– produces progesterone, estradiol, and inhibin A
– remains of ovarian follicle after ovulation
– inhibits release of gonadotropin-releasing hormone and luteinizing hormone
– new corpus luteum forms with each menstrual cycle
– size ranges from under 2 cm to 5 cm in diameter
– develops from follicular cells
– produces progesterone from cholesterol
– increase in enzyme P450scc during corpus luteum development
– involved in metabolism and produces antioxidant enzymes
– secretes progesterone and relaxin
– responsible for development and maintenance of endometrium and softening of pubic symphysis
– if egg is not fertilized, corpus luteum degenerates into scar tissue
– if egg is fertilized, corpus luteum continues to secrete progesterone
– prostaglandins can cause degeneration of corpus luteum and abortion of fetus
– in placental animals like humans, placenta takes over progesterone production
– luteal support involves administration of medication (progestins)
– corpus luteum gets yellow color from carotenoids, particularly lutein
– temporary endocrine structure in female mammals that forms after ovulation
– carotenoids concentrated from animal’s diet
– similar structures and functions in some reptiles
– dairy cattle follow similar cycle
– mentions pathology of corpus luteum cyst
– yellow hormone-secreting body in female reproductive system
– formed in ovary after ovulation
– made up of lutein cells
– secretes estrogens and progesterone
– prepares uterus for implantation and nourishment of embryo
– becomes inactive after 10-14 days if egg is not fertilized
– leads to menstruation.