In the intricate world of women’s health, there exists a realm of conditions and procedures that can often seem complex and confusing.
One such term, simple hyperplasia of endometrium, may leave you scratching your head.
But fear not!
Today, we embark on a journey through the fascinating realm of women’s health, exploring the enigmatic world of hyperplasia, endometrial biopsy, hormone therapy, and so much more.
Get ready to delve into a world where ovaries reign, hormones dance, and the mysteries of the menstrual cycle unfold.
So, hold on tight as we unravel the secrets of women’s health and leave no stone unturned.
simple hyperplasia of endometrium
Simple hyperplasia of the endometrium is a condition characterized by the thickening of the lining of the uterus.
It is typically diagnosed through an endometrial biopsy, where a sample of tissue is examined under a microscope.
Treatment options for simple hyperplasia may include hormone therapy, hysterectomy, or hysteroscopy.
This condition is often associated with menstrual cycle irregularities and can occur during perimenopause or menopause.
A transvaginal ultrasound exam may be used to further assess the condition.
Key Points:
- Simple hyperplasia of the endometrium is marked by thickening of the uterus lining.
- Diagnosis is usually done through an endometrial biopsy, with examination under a microscope.
- Treatment options include hormone therapy, hysterectomy, or hysteroscopy.
- It is commonly linked to menstrual cycle irregularities and can occur during perimenopause or menopause.
- A transvaginal ultrasound exam may be used for additional assessment.
- It is a condition of the uterus characterized by thickening of the lining and can be diagnosed via biopsy and treated by hormone therapy, hysterectomy, or hysteroscopy, typically in relation to menstrual cycle irregularities during perimenopause or menopause, sometimes assessed using transvaginal ultrasound.
simple hyperplasia of endometrium – Watch Video
💡
Pro Tips:
1. Simple hyperplasia of the endometrium: Trivia Edition!
1. Did you know that simple hyperplasia of the endometrium is often caused by an excess of estrogen? The overstimulation of the uterine lining can lead to an abnormal thickening and growth, resulting in this condition.
2. Simple hyperplasia of the endometrium is usually considered a non-cancerous condition. However, if left untreated and allowed to progress, there is a small risk of it developing into endometrial cancer, so it is essential to monitor and treat it accordingly.
3. Women with polycystic ovary syndrome (PCOS) are at a higher risk of developing simple hyperplasia of the endometrium due to hormone imbalances. Regular check-ups and hormone management can help prevent its occurrence.
4. Simple hyperplasia of the endometrium, while more common after menopause, can also occur in women of reproductive age. Irregular or heavy menstrual bleeding might be an indicator, so it’s crucial to consult a healthcare professional if any concerns arise.
5. In some cases, simple hyperplasia of the endometrium can regress on its own without any medical intervention. However, personalized treatment plans, such as hormonal therapy or minimally invasive procedures, might be recommended to promote healing and prevent further complications.
Simple Hyperplasia Of Endometrium
Simple hyperplasia of the endometrium is a condition characterized by the thickening of the lining of the uterus. The endometrium, which is the innermost layer of the uterus, normally undergoes changes throughout the menstrual cycle to prepare for possible pregnancy. However, in cases of simple hyperplasia, the endometrium becomes excessively thickened, leading to an imbalance in the normal hormonal regulation of the uterus.
This condition is typically caused by an excess of estrogen, a female hormone responsible for the growth and development of the endometrium. When estrogen levels are too high or remain unopposed by progesterone, the endometrium can continue to grow and thicken, resulting in simple hyperplasia.
While simple hyperplasia is usually not cancerous, it is important to identify and manage this condition to prevent it from progressing to a more severe form, such as atypical hyperplasia or endometrial cancer. Treatment options for simple hyperplasia may include hormonal therapy, endometrial biopsy, or in some cases, surgery.
Endometrial Biopsy
An endometrial biopsy is a diagnostic procedure commonly used to evaluate the health of the endometrium. During this procedure, a small amount of tissue from the lining of the uterus is collected and examined under a microscope. The biopsy helps in determining the presence of abnormal cells, assessing the thickness of the endometrium, and identifying the cause of any unusual symptoms.
This procedure is often performed in cases of abnormal uterine bleeding, suspected endometrial abnormalities, or to assist in the diagnosis of conditions such as simple hyperplasia. It is usually performed as an outpatient procedure, where a thin tube or suction device is inserted through the cervix to obtain a tissue sample.
Endometrial biopsy is a relatively quick and minimally invasive procedure that provides valuable information for diagnosing and managing various conditions affecting the endometrium, including simple hyperplasia.
Hormone Therapy
Hormone therapy involves the use of medications, such as estrogen and sometimes progestin, to relieve menopausal symptoms and manage certain hormonal imbalances. In the case of simple hyperplasia of the endometrium, hormone therapy may be prescribed to regulate the growth and shedding of the uterine lining.
Estrogen therapy is often administered to alleviate symptoms associated with menopause, such as hot flashes and vaginal dryness. However, in cases of simple hyperplasia where there is an excess of estrogen, progestin may also be prescribed to counteract the proliferative effects of estrogen on the endometrium.
It is important to note that hormone therapy should be tailored to each individual’s specific needs and may not be suitable for everyone. The decision to pursue hormone therapy for the treatment of simple hyperplasia should be made in consultation with an obstetrician-gynecologist (Ob-Gyn) who can assess the risks and benefits based on the individual’s medical history and overall health.
Hysterectomy
Hysterectomy is a surgical procedure in which the uterus is removed from the body. In cases of simple hyperplasia that do not respond to other treatment options or when there is concern for the progression to a more severe form of hyperplasia or endometrial cancer, a hysterectomy may be recommended as a definitive treatment.
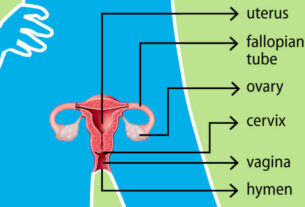
During a hysterectomy, the entire uterus can be removed, including the cervix, or in some cases, the cervix may be left intact. The decision regarding the removal of other structures, such as the ovaries and fallopian tubes, may also be made depending on the individual’s specific circumstances.
A hysterectomy is a major surgical procedure that requires careful consideration. It may have a significant impact on a woman’s reproductive capacity and hormonal balance. Therefore, a comprehensive discussion with an obstetrician-gynecologist is essential to explore all options and understand the potential benefits and risks associated with hysterectomy as a treatment for simple hyperplasia of the endometrium.
Hysteroscopy
Hysteroscopy is a procedure used to visualize and potentially treat abnormalities within the uterus. It involves the insertion of a lighted telescope, called a hysteroscope, through the cervix into the uterus. This allows the gynecologist to directly examine the uterine cavity and identify any structural or tissue abnormalities.
In cases of simple hyperplasia, hysteroscopy may be used to assess the thickness and appearance of the endometrium, as well as to obtain tissue samples for further analysis. The procedure can also be therapeutic, as certain abnormalities can be addressed during the hysteroscopy, such as removing polyps or performing endometrial ablation, which is the removal or destruction of the endometrium to reduce excessive bleeding.
Hysteroscopy is typically conducted as an outpatient procedure under local or general anesthesia. It is a minimally invasive technique that allows for precise diagnosis and potential treatment of various uterine conditions, including simple hyperplasia.
Menopause
Menopause is a natural biological process that signifies the permanent cessation of menstrual periods in a woman’s life. It is considered to be confirmed after one year of no menstrual periods. While menopause is a normal part of aging, it can also result from surgical removal of the ovaries or certain medical treatments.
During menopause, the ovaries gradually stop producing eggs and the levels of reproductive hormones, such as estrogen and progesterone, decline. This hormonal shift often leads to a variety of physical and emotional changes, including hot flashes, night sweats, mood swings, and vaginal dryness.
Understanding menopause is crucial in the context of simple hyperplasia, as this condition may be influenced by hormonal fluctuations associated with menopause. Regular check-ups with an obstetrician-gynecologist during this transitional phase can help identify and address any potential abnormalities, including simple hyperplasia of the endometrium.
Menstrual Cycle
The menstrual cycle refers to the monthly process of changes that occur in a woman’s body to prepare for the possibility of pregnancy. The typical menstrual cycle lasts between 21 and 35 days and involves a complex interplay of hormonal fluctuations.
During the menstrual cycle, the lining of the uterus, called the endometrium, undergoes cyclic changes. During the first half of the cycle, the ovaries produce estrogen, which stimulates the proliferation of the endometrium. This prepares the uterus for potential implantation of a fertilized egg.
If fertilization does not occur, hormone levels shift, leading to the shedding of the endometrial lining. This shedding results in menstrual bleeding, which typically lasts for a few days. Following menstruation, the cycle begins again with the reconstruction of the endometrium.
Understanding the menstrual cycle is essential to grasp the dynamics of simple hyperplasia, as an imbalance in hormonal regulation can disrupt the normal growth and shedding processes of the endometrium, contributing to the development of this condition.
Menstrual Periods
Menstrual periods, also known as menstruation or menses, refer to the shedding of blood and tissue from the lining of the uterus. Menstrual periods are a normal part of a woman’s reproductive cycle, occurring approximately every 21 to 35 days.
Menstrual bleeding usually lasts for several days, with the volume and duration varying from woman to woman. The color and consistency of menstrual blood may also differ throughout the cycle, ranging from bright red to dark brown.
In the context of simple hyperplasia of the endometrium, abnormal uterine bleeding may occur. This can manifest as heavy or prolonged periods, irregular bleeding between periods, or post-menopausal bleeding. Any changes in menstrual patterns should be promptly evaluated by an obstetrician-gynecologist to rule out underlying conditions, such as simple hyperplasia or other endometrial abnormalities.
Obstetrician-Gynecologist (Ob-Gyn)
An obstetrician-gynecologist (Ob-Gyn) is a medical specialist who focuses on women’s health, particularly in the areas of reproductive health, pregnancy, childbirth, and the management of disorders affecting the female reproductive system. Ob-Gyns play a crucial role in diagnosing and treating conditions such as simple hyperplasia of the endometrium.
These doctors receive specialized training in various aspects of women’s health, including gynecology (the study of the female reproductive system), obstetrics (the management of pregnancy and childbirth), and reproductive endocrinology (the study of hormones and their effects on fertility and reproductive health).
Ob-Gyns are skilled in performing diagnostic procedures, providing medical and surgical treatments, and offering guidance on preventive care and lifestyle modifications to optimize women’s health. Collaborating with an Ob-Gyn ensures comprehensive and personalized care for conditions such as simple hyperplasia of the endometrium.
Ovaries
The ovaries are two small organs located on either side of the uterus in women. They are responsible for producing and releasing eggs, or ova, for potential fertilization. Additionally, the ovaries produce and regulate the levels of reproductive hormones, including estrogen, progesterone, and androgens.
These hormones play a crucial role in the development and maintenance of secondary sexual characteristics, such as breast development and distribution of body fat. They also influence the menstrual cycle and contribute to the overall reproductive health of women.
In the context of simple hyperplasia of the endometrium, hormonal imbalances involving the ovaries can contribute to the thickening of the uterine lining. Conditions such as polycystic ovary syndrome (PCOS), characterized by hormonal disturbances affecting menstrual periods, ovulation, fertility, and metabolism, may increase the risk of developing simple hyperplasia. Managing ovarian function and hormonal balance is essential in the treatment and prevention of simple hyperplasia.
Hormone Therapy
Hormone therapy involves the use of medications, such as estrogen and sometimes progestin, to relieve menopausal symptoms and manage certain hormonal imbalances. In the case of simple hyperplasia of the endometrium, hormone therapy may be prescribed to regulate the growth and shedding of the uterine lining.
Estrogen therapy is often administered to alleviate symptoms associated with menopause, such as hot flashes and vaginal dryness. However, in cases of simple hyperplasia where there is an excess of estrogen, progestin may also be prescribed to counteract the proliferative effects of estrogen on the endometrium.
It is important to note that hormone therapy should be tailored to each individual’s specific needs and may not be suitable for everyone. The decision to pursue hormone therapy for the treatment of simple hyperplasia should be made in consultation with an obstetrician-gynecologist (Ob-Gyn) who can assess the risks and benefits based on the individual’s medical history and overall health.
Hysterectomy
Hysterectomy is a surgical procedure in which the uterus is removed from the body. In cases of simple hyperplasia that do not respond to other treatment options or when there is concern for the progression to a more severe form of hyperplasia or endometrial cancer, a hysterectomy may be recommended as a definitive treatment.
During a hysterectomy, the entire uterus can be removed, including the cervix, or in some cases, the cervix may be left intact. The decision regarding the removal of other structures, such as the ovaries and fallopian tubes, may also be made depending on the individual’s specific circumstances.
A hysterectomy is a major surgical procedure that requires careful consideration. It may have a significant impact on a woman’s reproductive capacity and hormonal balance. Therefore, a comprehensive discussion with an obstetrician-gynecologist is essential to explore all options and understand the potential benefits and risks associated with hysterectomy as a treatment for simple hyperplasia of the endometrium.
- Hysterectomy is a surgical procedure for removing the uterus
- It may be recommended for simple hyperplasia that doesn’t respond to other treatments
- The cervix may or may not be removed during the procedure
- Decision about ovary and fallopian tube removal depends on the individual
- Consultation with an obstetrician-gynecologist is crucial before opting for a hysterectomy.
Hysteroscopy
Hysteroscopy is a procedure used to visualize and potentially treat abnormalities within the uterus. It involves the insertion of a lighted telescope, called a hysteroscope, through the cervix into the uterus. This allows the gynecologist to directly examine the uterine cavity and identify any structural or tissue abnormalities.
In cases of simple hyperplasia, hysteroscopy may be used to assess the thickness and appearance of the endometrium, as well as to obtain tissue samples for further analysis. The procedure can also be therapeutic, as it allows for the removal of polyps or performing endometrial ablation, which is the removal or destruction of the endometrium to reduce excessive bleeding.
Hysteroscopy is typically conducted as an outpatient procedure under local or general anesthesia. It is a minimally invasive technique that allows for precise diagnosis and potential treatment of various uterine conditions, including simple hyperplasia.
- Benefits of hysteroscopy:
- Direct visualization of the uterine cavity
- Identification of structural or tissue abnormalities
- Assessment of endometrial thickness and appearance
- Tissue sampling for further analysis
- Therapeutic interventions, such as polyp removal and endometrial ablation
“Hysteroscopy is a valuable tool in gynecology for both diagnosis and treatment of uterine abnormalities.”
Menopause
Menopause is a natural biological process that signifies the permanent cessation of menstrual periods in a woman’s life. It is considered to be confirmed after one year of no menstrual periods. While menopause is a normal part of aging, it can also result from surgical removal of the ovaries or certain medical treatments.
During menopause, the ovaries gradually stop producing eggs and the levels of reproductive hormones, such as estrogen and progesterone, decline. This hormonal shift often leads to a variety of physical and emotional changes, including hot flashes, night sweats, mood swings, and vaginal dryness.
Understanding menopause is crucial in the context of simple hyperplasia, as this condition may be influenced by hormonal fluctuations associated with menopause. Regular check-ups with an obstetrician-gynecologist during this transitional phase can help identify and address any potential abnormalities, including simple hyperplasia of the endometrium.
Menstrual Cycle
The menstrual cycle refers to the monthly process of changes that occur in a woman’s body to prepare for the possibility of pregnancy. The typical menstrual cycle lasts between 21 and 35 days and involves a complex interplay of hormonal fluctuations.
During the menstrual cycle, the lining of the uterus, called the endometrium, undergoes cyclic changes. During the first half of the cycle, the ovaries produce estrogen, which stimulates the proliferation of the endometrium. This prepares the uterus for potential implantation of a fertilized egg.
If fertilization does not occur, hormone levels shift, leading to the shedding of the endometrial lining. This shedding results in menstrual bleeding, which typically lasts for a few days. Following menstruation, the cycle begins again with the reconstruction of the endometrium.
Understanding the menstrual cycle is essential to grasp the dynamics of simple hyperplasia, as an imbalance in hormonal regulation can disrupt the normal growth and shedding processes of the endometrium, contributing to the development of this condition.
- The menstrual cycle lasts between 21 and 35 days.
- Estrogen stimulates the proliferation of the endometrium.
- Menstrual bleeding typically lasts for a few days.
- Imbalance in hormonal regulation can lead to simple hyperplasia.
“Understanding the menstrual cycle is essential to grasp the dynamics of simple hyperplasia.”
Menstrual Periods
Menstrual periods, also known as menstruation or menses, refer to the shedding of blood and tissue from the lining of the uterus. Menstrual periods are a normal part of a woman’s reproductive cycle, occurring approximately every 21 to 35 days.
Menstrual bleeding usually lasts for several days, with the volume and duration varying from woman to woman. The color and consistency of menstrual blood may also differ throughout the cycle, ranging from bright red to dark brown.
In the context of simple hyperplasia of the endometrium, abnormal uterine bleeding may occur. This can manifest as heavy or prolonged periods, irregular bleeding between periods, or post-menopausal bleeding. Any changes in menstrual patterns should be promptly evaluated by an obstetrician-gynecologist to rule out underlying conditions, such as simple hyperplasia or other endometrial abnormalities.
- Menstrual periods involve the shedding of blood and tissue from the uterus lining.
- They occur approximately every 21 to 35 days.
- Menstrual bleeding can vary in volume and duration.
- The color of menstrual blood may range from bright red to dark brown.
- Abnormal uterine bleeding, such as heavy or prolonged periods, irregular bleeding between periods, or post-menopausal bleeding, may indicate underlying conditions.
- Prompt evaluation by an obstetrician-gynecologist is recommended for any changes in menstrual patterns.
Obstetrician-Gynecologist (Ob-Gyn)
An obstetrician-gynecologist (Ob-Gyn) is a medical specialist who focuses on women’s health, particularly in the areas of reproductive health, pregnancy, childbirth, and the management of disorders affecting the female reproductive system. Ob-Gyns play a crucial role in diagnosing and treating conditions such as simple hyperplasia of the endometrium.
These doctors receive specialized training in various aspects of women’s health, including gynecology (the study of the female reproductive system), obstetrics (the management of pregnancy and childbirth), and reproductive endocrinology (the study of hormones and their effects on fertility and reproductive health).
Ob-Gyns are skilled in performing diagnostic procedures, providing medical and surgical treatments, and offering guidance on preventive care and lifestyle modifications to optimize women’s health. Collaborating with an Ob-Gyn ensures comprehensive and personalized care for conditions such as simple hyperplasia of the endometrium.
Ovaries
The ovaries are two small organs located on either side of the uterus in women. They are responsible for producing and releasing eggs, or ova, for potential fertilization. Additionally, the ovaries produce and regulate the levels of reproductive hormones, including estrogen, progesterone, and androgens.
These hormones play a crucial role in the development and maintenance of secondary sexual characteristics, such as breast development and distribution of body fat. They also influence the menstrual cycle and contribute to the overall reproductive health of women.
In the context of simple hyperplasia of the endometrium, hormonal imbalances involving the ovaries can contribute to the thickening of the uterine lining. Conditions such as polycystic ovary syndrome (PCOS), characterized by hormonal disturbances affecting menstrual periods, ovulation, fertility, and metabolism, may increase the risk of developing simple hyperplasia.
Managing ovarian function and hormonal balance is essential in the treatment and prevention of simple hyperplasia.
- The ovaries produce and release eggs for potential fertilization.
- The ovaries produce and regulate reproductive hormones.
- Hormonal imbalances involving the ovaries can contribute to the thickening of the uterine lining.
- Polycystic ovary syndrome (PCOS) increases the risk of developing simple hyperplasia.
- Managing ovarian function and hormonal balance is crucial in the treatment and prevention of simple hyperplasia.
“Managing ovarian function and hormonal balance is essential in the treatment and prevention of simple hyperplasia.”
💡
You may need to know these questions about simple hyperplasia of endometrium
What is simple endometrial hyperplasia?
Simple endometrial hyperplasia is a common precancerous condition characterized by an abnormal thickening of the uterine lining. While it may not initially present with severe symptoms, it can lead to discomfort such as heavy menstrual periods, postmenopausal bleeding, and anemia due to excessive blood loss. It is crucial to address this condition promptly through appropriate medical interventions to prevent its progression to cancer.
Can simple endometrial hyperplasia turn into cancer?
Simple endometrial hyperplasia has a slight possibility of progressing into cancer. While the most common type, known as mild or simple hyperplasia, carries a very low risk, it is important to monitor and treat it accordingly. In some cases, this hyperplasia may resolve spontaneously or with hormone therapy. However, if the hyperplasia is classified as “atypical,” the likelihood of it developing into cancer increases. Therefore, it is crucial to closely monitor and manage any atypical endometrial hyperplasia cases to prevent further complications.
Is endometrial hyperplasia serious?
Untreated endometrial hyperplasia, especially the atypical type, can result in serious consequences. Atypical endometrial hyperplasia carries a risk of developing into endometrial or uterine cancer, particularly if left untreated. Studies have shown that approximately 8% of individuals assigned female at birth with untreated simple atypical endometrial hyperplasia may develop cancer. Furthermore, the risk increases significantly to nearly 30% for those with complex atypical endometrial hyperplasia who do not receive appropriate treatment. Therefore, it is crucial to address endometrial hyperplasia promptly to mitigate the potential seriousness of the condition.
What is the first line treatment for endometrial hyperplasia?
The first-line treatment for endometrial hyperplasia without atypia is either continuous oral progestogens or the levonorgestrel-releasing intrauterine system (LNG-IUS). Both of these options have been proven to effectively achieve regression of endometrial hyperplasia without any atypia. Continuous oral progestogens or the LNG-IUS can be considered as the primary medical treatment for this condition.
Reference source
https://www.acog.org/womens-health/faqs/endometrial-hyperplasia
https://www.yalemedicine.org/conditions/endometrial-hyperplasia
https://www.cancer.org/cancer/types/endometrial-cancer/causes-risks-prevention/risk-factors.html
https://my.clevelandclinic.org/health/diseases/16569-atypical-endometrial-hyperplasia