Understanding the Challenges of a Generally Contracted Pelvis: Exploring Birth Complications and Solutions
– Contracted pelvis is rare in developed countries but is still prevalent in some developing countries.
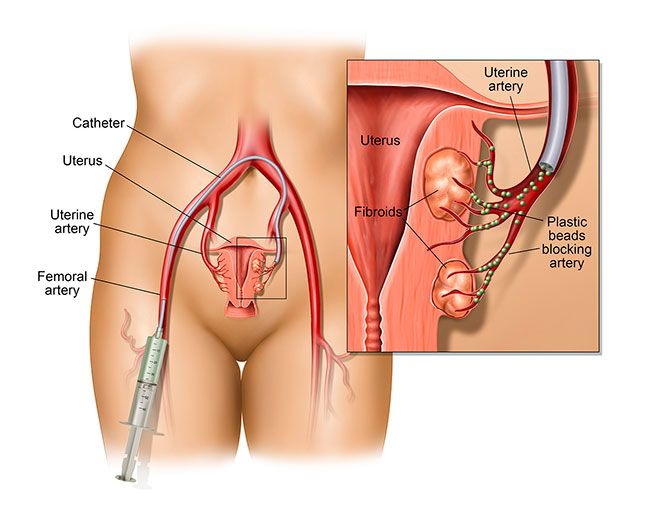
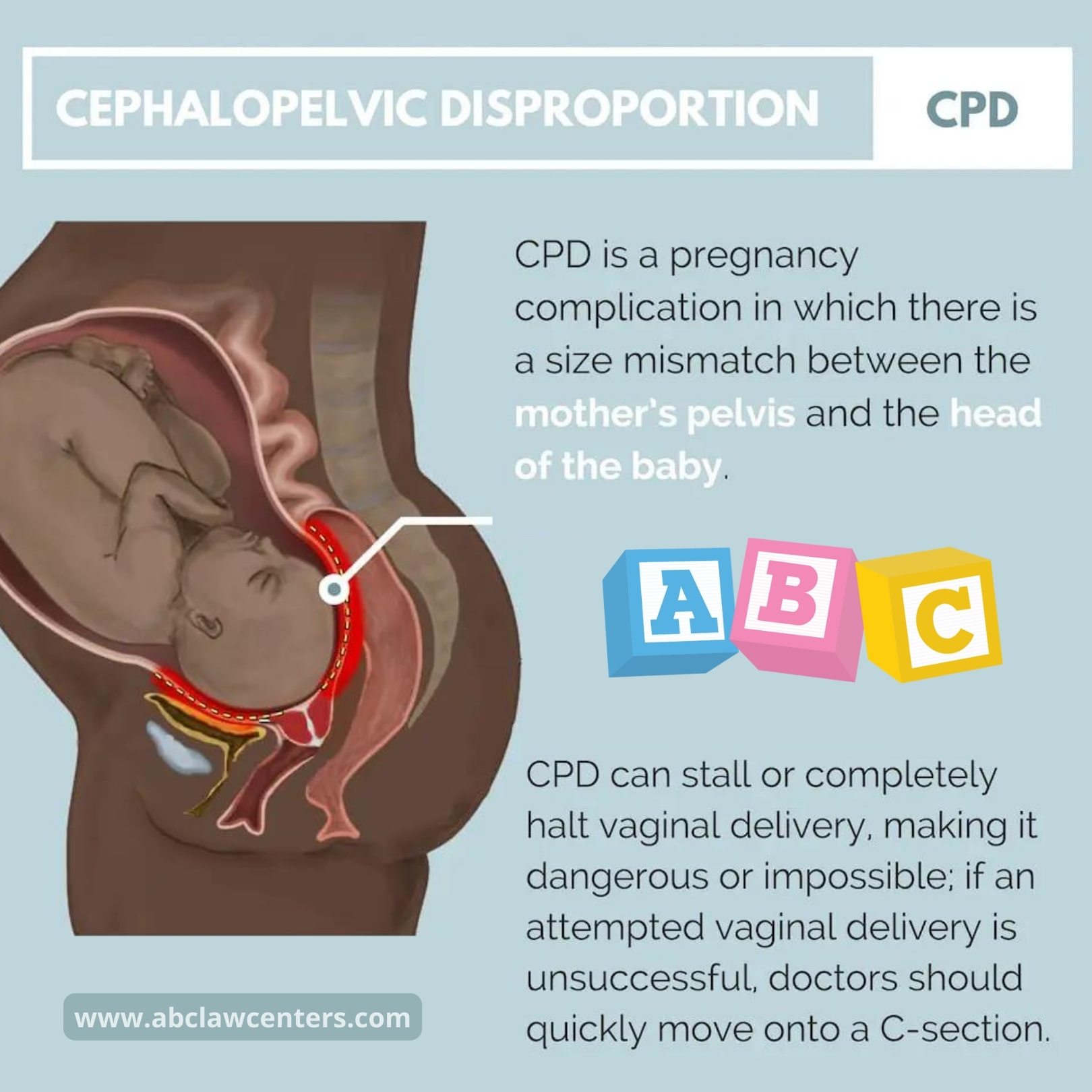
– Contracted pelvis is the major cause of cephalopelvic disproportion, Labour Dystocia, and instrumental delivery.
– Labour Dystocia is the most common complication associated with a contracted pelvis and can lead to increased incidence of perinatal and maternal morbidity and mortality.
– The shape, type, and diameter of the female pelvis determine the course and outcome of labor.
– The pelvis is made up of the sacrum, coccyx, and two os coxae (ischium, ilium, and pubis).
– The pelvic cavity is divided into the true pelvis and false pelvis by the pelvic inlet.
– The pelvic inlet involves three units of the bone pelvis (first sacral segment, iliac and pubis portion).
– The shape of the pelvic inlet depends on the general shape of the pelvis, which can be classified into gynaecoid, android, anthropoid, and platypelloid types.
– The gynaecoid pelvis is the most suitable for a vaginal birth, while the android and platypelloid pelvis types are suboptimal.
– The anteroposterior (or “conjugate”) diameter of the pelvic inlet is important and can be measured as the anatomical conjugate, obstetric conjugate, and diagonal conjugate.
– A contracted pelvis is established when the pelvic inlet at the interaxial dimension is less than 10 cm.
– Developmental, metabolic, traumatic, neoplastic, and lumbar kyphosis factors can contribute to a contracted pelvis.
– Diagnosis methods for contracted pelvis include abdominal examination, pelvimetry (internal and external), and imaging pelvimetry using X-ray, CT, or MRI.
– Complications associated with contracted pelvis include pendulous abdomen, nonengagement, pyelonephritis, prolonged labor, rupture of membranes, cord prolapse, obstructed labor, birth asphyxia, fracture skull, nerve injuries, and intra-amniotic infection.
– The management of contracted pelvis depends on the degree of contraction, with vaginal delivery recommended for minor degree, trial labor for moderate degree, and caesarean section for severe or extreme degree.
– Physiotherapy interventions can be beneficial for minor and moderate contracted pelvis, focusing on postural changes to increase pelvic inlet diameters and aid in labor progress.